
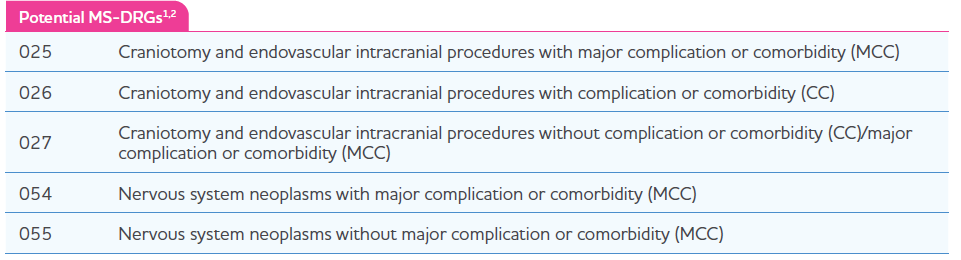
Medicare Severity Diagnosis Related Group (MS-DRG) Coverage
Similar to other inpatient administered drugs, Gleolan® will be bundled by payers into hospital payment rates (ie, MSDRGs), all patient refined (APR DRGs), or other DRGs specific to the individual payer’s internal methodology. DRG assignment depends on the diagnosis and the craniotomy or craniectomy procedure with which Gleolan will be bundled. Medicare utilizes MS-DRGs; the 5 MS-DRGs that represent craniotomy or craniectomy treatments involving Gleolan are shown in the table below. This table may not be reflective of all MS-DRGs or other non–MS-DRGs that may be used for Gleolan. Only 1 MS-DRG should be assigned to a patient for a particular hospital admission.
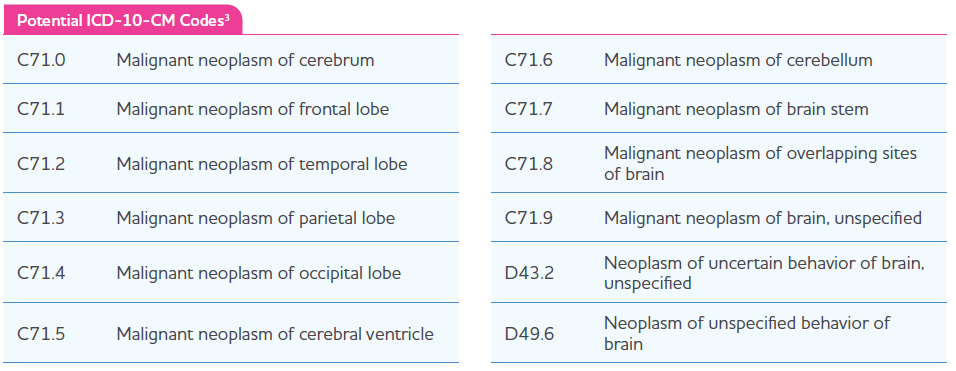
ICD-10 Clinical Modification (CM) Diagnosis Codes
Hospitals use current ICD-10-CM codes to report a patient’s diagnosis on claims forms. Correct coding is the responsibility of the hospital submitting a claim for the item or service. Always check payer guidelines to verify diagnosis coding requirements as individual payer rules may vary and must be adhered to. Below is a range of potential ICD-10-CM diagnosis codes that may be related to a diagnosis within Gleolan’s approved label.
ICD-10 Procedure Coding System (PCS) and Revenue Code
Effective 01/01/2019, the Centers for Medicare & Medicaid Services (CMS) created a new PCS code that captures the PCS method value Fluorescence Guided Procedure and the PCS qualifier value Aminolevulinic Acid and applies them to the fourth character body region values and applicable approaches. These changes enable the capture of additional detail for fluorescence-guided procedures that use aminolevulinic acid. The ICD-10-CM/PCS Coding Clinic Fourth Quarter 2019, pages 41 to 42, confirms the utilization of code 8E090EM for Fluorescence Guided Procedure of Head and Neck Region Using Aminolevulinic Acid, Open Approach. For additional information, please consult the current ICD-10-PCS manual. Some individual payers may require specific accommodations for billing imaging agents on inpatient claims. Always confirm adherence to specific payer rules and guidelines.

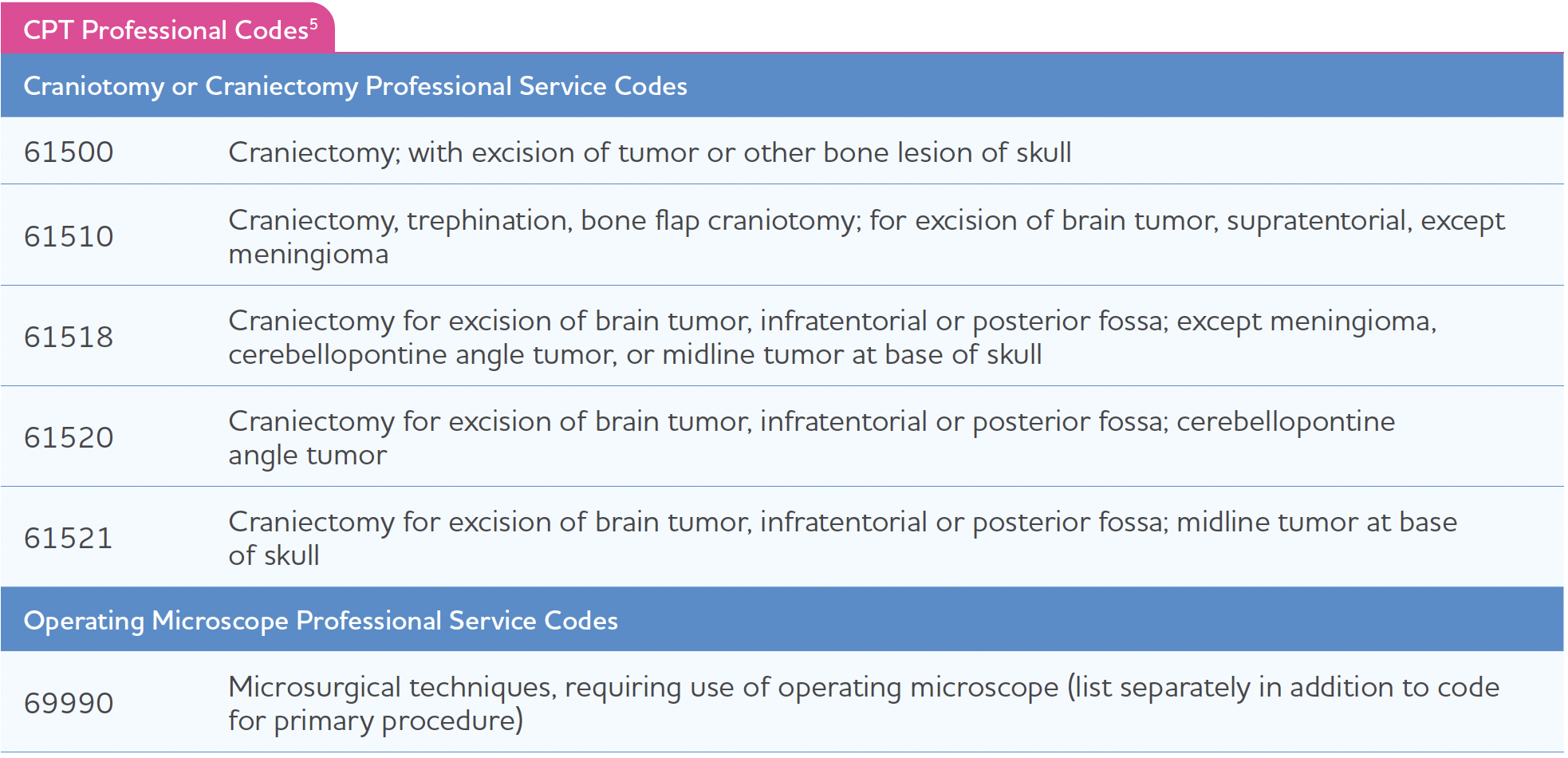
Professional Current Procedural Terminology (CPT) Codes
In addition to facility inpatient reimbursement, some hospitals also bill out professional physician fees separate from the inpatient procedure. Craniotomy and craniectomy procedures will vary. The below list is meant to serve as a guide of commonly used professional fees; however, it is not exhaustive, and individual circumstances and payer rules will determine coding.
Each payer can have unique requirements for their claims process. Please consult with the payer to ensure compliance with their requirements.
Obtain more information on reimbursement support by calling 1-833-433-9833, from 9:00 am to 5:00 pm EST Monday through Friday (excluding holidays).
